
Popular Tags
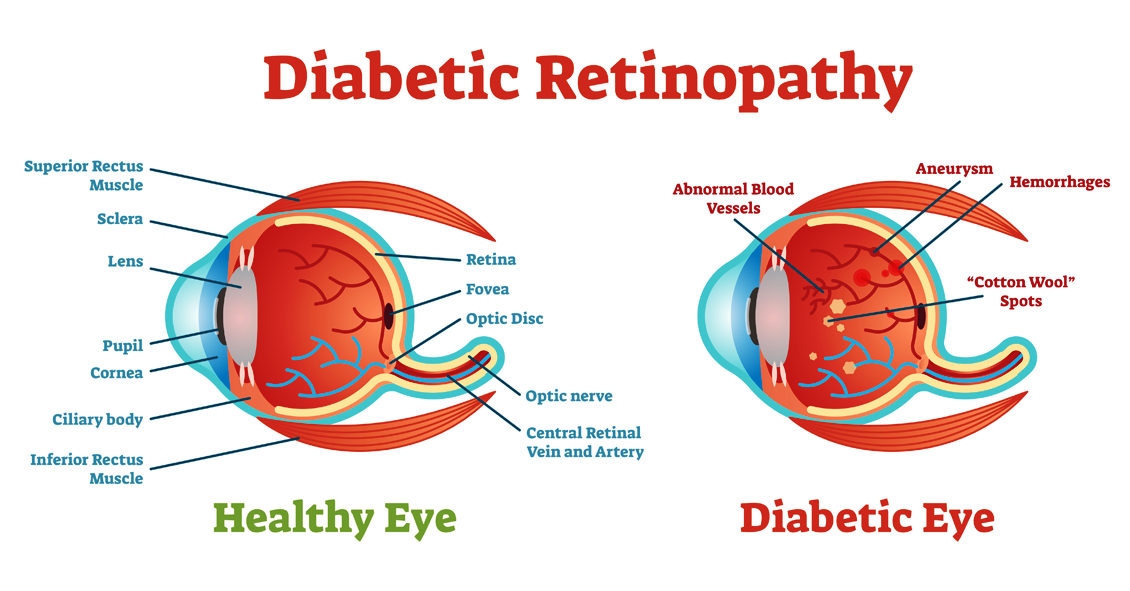
Diabetic retinopathy is an eye condition that affects the retina in people who have diabetes.
The retina is the light-sensitive tissue that lines the back of the eye, and detects light that is then processed as an image by the brain....
Visual Field
The visual field test is designed to see how well you see outside of the center part of your vision (peripheral vision).
When we test your vision on the basic eye chart it is only testing how well you see right in the center...

Fall brings a lot of fun, with Halloween bringing loads of it.
But did you know that some Halloween practices could harm your vision? Take Halloween contacts for instance. They are wildly fun with everything to monster eyes, goblin eyes, cat...